Artificial Disc Replacement Models
Artificial Disc Replacement: Definition
Artificial Disc Replacement, also known as artificial disk replacement and total disc replacement (TDR), refers to the artificial disc replacement surgery and to the man-made device, which replaces the entire function of the diseased or damaged intervertebral disc of the spinal column. The Artificial Disc Replacement (ADR) was developed to overcome the shortcomings of older fusion technology, which is associated with reduced flexibility, poor success rates, high re-operation rates and adjacent segment syndrome. See patient video stories about Artificial Disc Replacement and written stories about Dr. Bertagnoli Reviews
ADR design classification can be broken down into two types, those with the a fixed Center of Rotation (COR) and those with a movable (COR). Of those with a movable COR they can be broken down into design groups, elastomer, or as some say rubbery, cores and those with a semi-spherical core. Prof. Dr. Bertagnoli has experience (6,000 ADR implants and 10,000 anterior/ventral approaches) with all of these disc types (at the time of this writing perhaps 30 have been developed), as he is often sought by ADR manufacturers for his experience and expertise. And after all these surgeries, he has developed a decided preference for ADRs with a fixed center of rotation. In his opinion these type of discs yield longer lasting results with fewer complications, especially avoiding complications with the facet joints. Movable (COR) often do not perform as expected in the human body and their promised additional benefits have not yet been measured in real patients. For more discussion about disc types please see Artificial Disc Replacement - Center of Rotation
Artificial Disc Replacement: Indications
Artificial Disc Replacement: Contraindications
- Idopathic or severe degenerative scoliosis with marked rotation. (In degenerative scoliosis ADR in combination with DPI techniques can address the condition.)
- Fresh fractures in the proposed surgical area
- Tumors in the proposed surgical area
- Pars defect
- Spondylolisthesis > Grade 1 (degenerative pseudoolisthesis is not a contraindication – ADR will realign this secondary slip if the spondylothisthesis is grade one or below)
- Pregnancy (for the lumbar ADR)
- Active infection
Artificial Disc Replacement: Disc Choice
Prof. Dr. Bertagnoli will advise the patient on the pros and cons of these devices, based on long term outcomes and the patients individual condition. In this burgeoning new world of spine arthroplasty, ADRs are being sent to market every month, but what is new may or may not be the best. The vast majority of these devices are rejected by the professor. To learn more see clickcomparisons of ADR designs
Artificial Disc Replacement: Cervical
CLICK THE NAME FOR A LARGER PICTURE
Current cervical artificial disc replacements available in Europe are the:
 Activ C
Activ C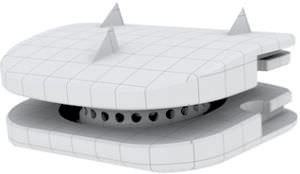 Baguera C
Baguera C BioLign
BioLign Bryan
Bryan Cervicore
Cervicore CP-ESP
CP-ESP CSpsineDisc
CSpsineDisc Discovery
Discovery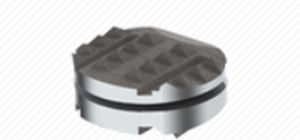 DyanlisC
DyanlisC Freedom cervical disc
Freedom cervical disc Granvia-C
Granvia-C Kineflex-C
Kineflex-C Mobi-C
Mobi-C PCM (Porous Coated Motion)
PCM (Porous Coated Motion) Physiodisc
Physiodisc  Prestige
Prestige Prodisc-C
Prodisc-C Prodisc-C Nova
Prodisc-C Nova Prodisc-C Vivo
Prodisc-C Vivo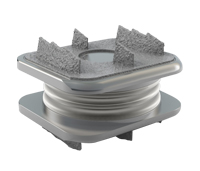 Spinal Kinetics M6-C
Spinal Kinetics M6-C Secure-C
Secure-C
*Prof. Dr. Bertagnoli does not necessarily recommend every device listed here.
Artificial Disc Replacement: Lumbar
 Activ-L
Activ-L Charite
Charite Flexicore
Flexicore Freedom Lumbar Disc
Freedom Lumbar Disc LP-ESP Click name for large picture
LP-ESP Click name for large picture Maverick
Maverick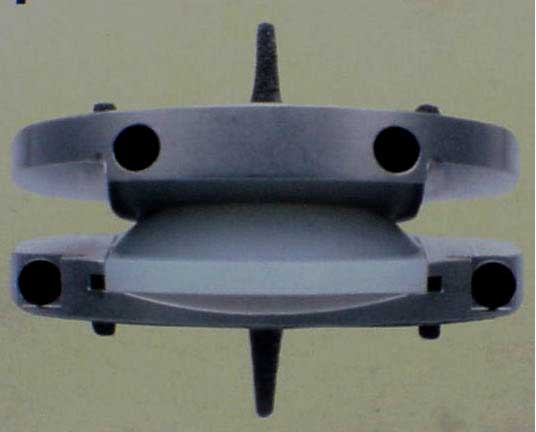 Prodisc-L Click name for large picture
Prodisc-L Click name for large picture Prodisc-Oblique or Prodisc-O Click name for large picture
Prodisc-Oblique or Prodisc-O Click name for large picture Spinal Kinetics M6-L
Spinal Kinetics M6-L
*Prof. Dr. Bertagnoli does not necessarily recommend every device listed here.
Artificial Disc Replacement: Surgery
Artificial Disc Replacement surgery techniques are very similar between devices. This is because the steps for implantation and the instrumentation for implantation are quite similar and many of these standards were established by Prof. Dr. Bertagnoli. The greatest difference in surgical steps is the whether or not the device is in one or two or three parts and whether or not the device uses spikes, keels or nodules. There are advantages and disadvantages of these approaches. Both Cervical Artificial Disc Replacement and Lumbar Artificial Disc Replacement require a ventral (front/anterior) incision, with the exception of the Prodisc-O, the Nuvasive lumbar discs, which represent special spine cases in the lumbar. The patient should also be aware that not all doctors do this surgery in the same manner. The safety and likelihood of a good outcome are based in the fundamental steps a surgeon takes.
Artificial Disc Replacement: Surgery Risks
All surgery carries risks from anesthesia, blood clots and infections. If complications from these risks arise, they most often can be successfully treated. The physical condition of the patient (such as obesity and diabetes) can also add risk to surgery.
Artificial Disc Replacement: Surgery Long-Term Outlook
The appropriate surgical procedure properly executed will provide long-term relief for the degenerated disc(s) treated. However, if the condition was allowed to continue too long and the nerves have become damaged, there may be some remaining pain or numbness or no improvement. Also, any degenerative process will likely continue, therefore problems in other areas of the spine may appear at a later time.
Artificial Disc Replacement
