Artificial Disc Replacement - Center of Rotation
This page was originally designed to discuss only the dynamics of motion in artificial disc design, but other important issues outside of the motion of the discs have arisen in the years coinciding with the onset of elastomer discs (Spinal Kinetics M6 and many others) and movable core discs (like the Charite' and others) have been added to the discussion. Essentially this page explains that elastomer and/or movable core discs have more risk of complications than fixed core ADRs and that there is no evidence of promised superior benefits, only speculation. We are focused on long-term proven, results in the human body. Hyperbolic, unproven promises of marketers and those manufacturers seeking to enter this section of medicine, especially in the USA, should be viewed with great skepticism by the patient.
- Deceptive Advertising by some Doctors
- Center of Rotation (COR) in the Coronal Plane
- COR in Spondylolisthesis and L5/S1
- Sizing
- Bent Shoe Syndrome
- Sagittal Translation
- Cushioning is not Pain Relief
- The Ideal is not the Real Situation
- Axial Rotation
- Kinematic Analysis
- No FDA Approval of Elastomer Discs
- Trauma to Elastomer Discs
- Durability Counts
- Class Action Lawsuits
- Movable Core/Ball Discs
--------------------------------------------------------------------
- Deceptive Advertising by Doctors
Sadly we must begin with saying that we have documented some marketers in cooperation with doctors and doctors alone advertising as if they are Prof. Dr. Bertagnoli or that Prof. Dr. Bertagnoli supervises their surgery. They also imply in their ad headline that Prof. Dr. Bertagnoli endorses the M6 or this doctor. This is TOTALLY false on both counts. When the patient clicks on the ad they are then directed to another doctor's webpage. We find this despicable that some would treat the serious nature of a patient's health with deception and beyond the bounds of ethical behavior for a doctor. Please see one example below.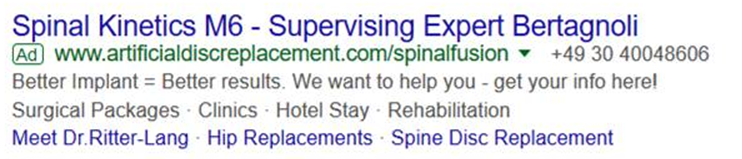

- Center of Rotation (COR) in the Coronal Plane
The Center Of Rotation (COR) is an important concept in artificial disc replacement surgery and it is often misunderstood. To understand this concept we should begin with identifying the direction of rotation in question. After all, the spine moves in many directions, but it is the flexing forward and extending backwards, which is our primary concern. This is because this motion affects the facet joints, when they are under the greatest pressure. In the natural healthy patient the Center Of Rotation (COR) is posterior to the center of the vertebra about one third of the diameter of vertebrae from the posterior edge; however to date, all artificial discs are unable to reconstruct the exact natural Center Of Rotation (COR). However, a properly placed and sized semi-constrained device (ball-and-socket design) can very closely approximate this position and maintain it. This analysis, Motion Path of the Instant Center of Rotation, published in the prestigious Spine journal clearly supports the need for controlling the center of rotation and precise placement of the artificial disc at each level. An elastomer disc cannot do this as it relies on usually compromised structures around the disc to guide the movement of the disc. (Axial or side-to-side rotations (discussed later) or the twisting of the back is controlled by muscles and limited by the facet surfaces at their maximum surface exposure, unlike the extension position where wedging takes place, causing maximal force on the surface of the facets.)
Semi-constrained devices control the center of rotation of the ADR and prevent undue stress on the facets in the extension motion. This is especially true in multi-level ADR surgery, where multiple segments are affected. This corrective measure is needed in most spine patients, because of the imbalances in the spine caused by long-term conditions and because some surrounding tissue are often resected (cut away) during surgery, leaving fewer guiding structures for the movement of the disc. (Prof. Dr. Bertagnoli preserves these structures whenever possible, unlike other surgeons who call them unnecessary.) It is this concern about surrounding structures, which indicate that artificial disc replacements play a larger role than acting as a movable spacer, but one of maintaining spinal stability. Looking to the future, one must also consider the long-term destabilizing affects of spondylosis, which all patients with degenerative disc disease (DDD) have. This is yet another reason for the semi-constrained device. - COR in Spondylolisthesis and L5/S1
The lack of control of the center of rotation is also a reason elastomer discs should not be used in segments with a spondylolisthesis (less than grade 1) or in the l5s1 spinal intervertebral disc space, which is the segment of the spine with the greatest shear force. There is simply no way for these devices to maintain stability and the patient has a higher risk of device failure. - Sizing
Semi-constrained devices also are sized not only horizontally and vertically, but also for the expected curvature of the spine, providing more orthopedic correction and long-term stability. Most elastomer discs cannot do this. - Bent Shoe Syndrome
Also, in some elastomer discs we are observing microfractures in the "artificial annulus" within a year after implantation. This raises concern about a fast rate of debris shedding from the "artificial annulus". This has been nicknamed the "bent shoe syndrome". Just imagine bending a shoe a thousand times a day and what would happen to the material. Elastomer discs bend whereas semi-constrained discs glide across a core. Also, many of the chemicals used in these devices are unknown and their affect on the bones have not been completely studied, however there is clinical evidence to support the notion that their debris is causing osteolysis (the erosion of bone stock).
Breakage from constant bending of the material is another concern. Even with titanium rods we have seen breaks in patient spines after years of stress and bending, even though this bending is barely perceptible. What would be the effect on much larger bending on material made of unknown chemistry? See example of an Spinal Kinetics M6 failure posted by a patient.and this Scientific Article - Sagittal Translation
The lack of control by elastomer discs contributes to what is known as sagittal translation (instability or unstable motion transferred to horizontal/axial motion). (The deceptive marketers call this "adaptive") Spinal instability is mimicked by elastomer discs contributing to facet problems. Put another way, these discs do not restrict some of the instability of the spine nor do they offer any method to force the restoration of the natural position of vertebrae. They move according to the soft tissue structures about them, which are usually compromised by thickening and calcification. - Cushioning is not Pain Relief
Many patients believe that cushioning gives pain relief. This is simply not true. It is the decompression of the nerves and nerve roots that give pain relief. In fact most cushioning of the spine comes the flexing of the natural curve of the spine, which is controlled by the muscles. - The Ideal is not the Real Situation
Ideally, any disc would shift the Center Of Rotation (COR) like the natural disc. Indeed this is what is hoped by the designers of the elastomer discs. However, this would only be true if the vertebrae anchoring the elastomer disc and the surrounding supporting structures were perfectly patent or the surgeon perfectly remodeled the vertebrae and all the ligaments, tendons and muscles surrounding the affected level were balanced as they are in a complete healthy segment. Unconstrained/elastomer discs are fully dependent on these usually compromised surrounding structures for guidance of their motion like a natural disc. But balancing spinal column with elastomer discs is highly unlikely especially in a multilevel case, because the supporting structures have most likely adapted to the degenerative condition of the spine and have possibly calcified. Therefore, they would pull eventually the spine out of alignment and this could cause facet problems. If surrounding supporting structures are shortened and calcified, the surgeon would have to resect them, to allow for the regaining of balance. Such resections would not be desirable as it would further destabilize the spine. Hence, elastomer discs are adequate only in very selected cases in the short-term. - Axial Rotation
Horizontal/axial rotation (twisting of the spine) is dampened and controlled by muscles and eventually limited by the facet joints/spinal processes, which is the natural function of the facet joints. This is quite limited in the lumbar spine. The thoracic spine spine provides most of the twist. If you are relying on your artificial disc to do achieve this dampening, you are subjecting yourself to shearing forces in the worse possible motion direction. An elastomer disc has internal friction contributing to horizontal shearing forces, lowering the probability of boney in-growth of the prosthesis in the time shortly after the surgery and increasing the probability of migration of the disc. Hence it is undesireable to dampen horizontal rotation (twisting) with an ADR, as this is done naturally by the facets and supporting structures (such as the anterior and posterior ligaments and the intraspinous muscles), every day of a person's life. Some postings by non-doctor marketeers hyping elastomer discs misuse the term hypermobility to describe this motion. Hypermobility is used correctly to describe the condition of the spine segment with a disc, which has lost considerable disc height.
It is also misleading to say that the internal resistance of an elastomer disc is equivalent to the natural disc. It is misleading because the natural disc attaches to the vertebrae very differently than an artificial disc. Creating stress at this attachment point has its risks. - Kinematic Analysis
One kinematic analysis (sponsored by the manufacturer) puts a positive spin on elastomer discs in single level cases, but this engineering analysis does not take into account the vast complexities of the human spine's structure and the current condition of a patient's spine. These engineering "studies" assume perfect conditions and that no degeneration of the spine will occur in the future. Nor does this analysis consider multi-level cases. Such an analysis is inferior to en vivo long-term FDA IDE clinical STUDIES and is not the research standard in medicine. - FDA approval - Patents - What is Newer is Not Necessarily Better
The patent office grants patents to inventions which are sufficiently different to previous inventions.. They make no determination as to its safety or effectiveness. Hence newer is not necessarily better or for that matter works at all. For a medical device manufacturer to participate in the next wave in orthopedic surgery they must have a patent. This is expanded on in the book, The Danger Within Us: America's Untested, Unregulated Medical Device Industry and One Man's Battle to Survive It Hardcover – December 12, 2017. The FDA, to the limit of usually a five year trial, determines what is safe and effective. Despite being around for more than ten years, to date no elastomer disc has won FDA approval Indeed many devices and drugs fail FDA trials and their patients suffer as a result. Even after FDA success, devices and drugs are recalled. The patient should consider only devices with a long history after FDA approval. Choose something with a proven track record. The latest is not always the greatest. Many ADR designs have come and gone. Also it is very difficult for patients to get insurance reimbursement on a device that is not FDA approved. - Trauma to Elastomer Discs
Some supporters of elastomer discs say that three part disc are subject to subluxation, but this is only true if severe traumatic forces are applied. But the consequences of these traumatic forces on a singular modular unit could much more severe, such as tearing the unit from the bone. If the annulus is torn, then the internal contents are spilled into the body cavity. If the endplates of a unibody ADR are not torn away and the unibody disc needs replacement, then the unibody ADR must be chiseled away, whereas a three part ADR can simply have its core replaced. Chiseling away an ADR severely compromises the boney structures in a revision surgery. - Durability Counts
The patient should consider how well an artificial disc will perform in a traumatic situation. We expect our patients to live a full and active life after surgery, even though this might expose them, not only only to riskier situations, i.e. mountain biking, skiing, etc. but household accidents. Should such an accident occur, a properly designed disc greatly increases the chance of survival and the mitigation of complications by retaining the stability of the spine. This is more than speculation. For a real life story concerning such an accident please see Hangman's Fracture After ADR". Unibody elastomer discs could easily have been destroyed or torn from the vertebrae, increasing the likelihood of spinal cord damage. - Class Action Lawsuits
Some lawsuits are only nuisance lawsuits brought by often uninformed individuals and have no or little merit, but we think when attorneys form a class from past early patients and bring a class action lawsuit against an elastomer artificial disc manufacturer it adds merit our observations. - Movable Core/Ball Discs
Another concept in artificial disc design is the movable core, this design has the "ball", on which the socket moves over, sliding in a track based on the position of the vertebra above and below it, plus the weight distribution. This is done in the hopes of better mimicking the natural disc, but the reality is much different than the concept. In most cases the "ball' moves to one position and stays there. Which position it moves to depends on the condition of the already compromised spine. Now the spine, particularly the facet joints, is further stressed in the position not aligned for the frozen"ball", causing back pain. Indeed, a hypermobility and a resultant spondyloslihesis can be create as pointed out by this articles ==> Kerferd 2017 Hypermobility
Note: In some patients with severely damaged facets, 360 motion preservation can be a solution.
